The suicide of 16-year-old has spotlighted India’s surge in student suicides, revealing deep gaps in school accountability, mental-health systems, and a pressure-driven education culture that continues to overlook children’s emotional safety and dignity.
Alarming Data on Student Suicides in India
The latest National Crime Records Bureau (NCRB) data presents a grim and escalating picture of the crisis:
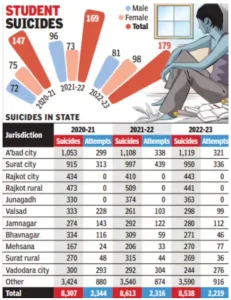
- Record Surge in Student Suicides: The number of student suicides hit a record 13,892 in 2023. This is a big 65% jump in the last ten years (from 8,423 in 2013), based on NCRB data.
- Outpacing the National Average: The rate of increase in student suicides is more than double the rise in the national overall suicide rate (27% over the last decade).
- This shows that young people are much more at risk.
- Dropping Age of Distress: The problem is starting earlier, with cases now found in the 9–17 age group, highlighting stress and neglect in schools at all levels.
- Regional Hotspots and Differences: High-population states like Maharashtra, Madhya Pradesh, Uttar Pradesh, and Tamil Nadu report the highest numbers.
- However, some states, like Kerala, have 80% compliance with rules, leading to a 12% drop in incidents. This is very different from states like Uttar Pradesh, where compliance is low.
- Acute Shortage of Mental Health Professionals: India has a severe lack of mental health experts, with only about 0.75 Psychiatrists per 100,000 people.
- This leaves a massive 70-92% gap in treatment for mental illnesses.
- Economic and Future Risks: The crisis threatens India’s productivity, with losses of one to two percent of Gross Domestic Product, approximately two and a half to five lakh crore rupees or thirty to sixty billion United States dollars annually. Without intervention, student suicides could exceed twenty thousand annually by 2032.
- Full adoption of the National Education Policy 2020, Social and Emotional Learning, and Supreme Court guidelines could reduce cases below eight thousand by 2035, reversing the trend by forty percent.
Causes of Student Suicide in India
The tragedy stems from a toxic interplay of academic pressure and systemic inequalities:
- Structural and Academic Pressures:
- Hyper-Competitive Academic Pressure: Intense competition in exams like NEET and JEE, fueled by the aggressive coaching culture, is a major psychological stressor, prioritizing marks over holistic mastery.
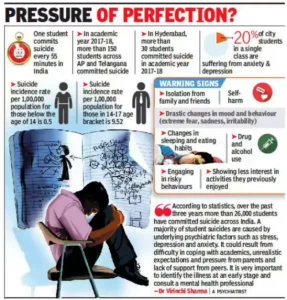
- This stress is acutely felt around exam periods, leading to clusters of suicides during exam months in states like Telangana and Uttar Pradesh.
 Institutional and Teacher Harassment: Recent cases highlight punitive institutional culture, where public shaming, bullying, and alleged harassment by teachers erode a student’s dignity.
Institutional and Teacher Harassment: Recent cases highlight punitive institutional culture, where public shaming, bullying, and alleged harassment by teachers erode a student’s dignity.- Bullying Normalisation: Verbal taunts, exclusion, and physical teasing are tragically trivialized as ‘normal teenage behaviour’ by staff, despite constituting severe adverse childhood experiences (ACEs).
- According to UNICEF’s Child and Adolescent Mental Health Service Mapping, India 2024 report, 6.46% of community children (assessed in their homes and neighbourhoods, not in schools) and 23.33% of schoolchildren and adolescents have psychiatric disorders.
- The National Mental Health Survey (2015-16) found that about eight to 11 million adolescents require mental health treatment at any given time.
- ACEs refer to stressful or traumatic events occurring before the age of eighteen that can severely disrupt a child’s emotional development, brain architecture, and long-term health outcomes.
- Digital Overstimulation: Social media’s dopamine cycle creates distorted self-image and heightens impulsivity, making distress management difficult.
- The mandatory high screen time during the pandemic and its aftermath has led to significant post-pandemic behavioral shifts, including social withdrawal, low emotional resilience, and chronic anxiety among adolescents.
- Intersectional Vulnerabilities:
- Caste and Class Marginalization: SC/ST/OBC students face 20-30% higher risk due to discrimination, reservation backlash, and economic precarity.
- Gender Disparities: Suicides among female students rose 7% (2021–22), reflecting patriarchal pressures, social stigma, reproductive health taboos, and marriage-related expectations—with girls accounting for 47% of total student suicides.
- Rural-Urban and LGBTQ+ Gaps: Rural suicides stem from limited counseling access, while queer youth face heightened vulnerability due to social stigma and familial rejection.
- Family-level Emotional Vacuum: The breakdown of joint families, coupled with parental work pressures, nuclearization, and digital distraction, creates an emotional vacuum where children internalize distress in silence.
Legal and Constitutional Foundations for Student Protection in India
India’s framework, though evolving, is now powerfully reinforced by the judiciary:
- National Strategy: The National Suicide Prevention Strategy (NSPS, 2022) aims to reduce suicide deaths by 10% by 2030.
- This target, however, lags behind the 33% reduction sought under SDG 3.4 for premature mortality.
- Helpline Service: Tele-MANAS provides free, 24/7 mental health support, taking over 29.75 lakh calls since it started.
Supreme Court’s ruling in Sukdeb Saha vs. State of Andhra Pradesh (July 2025)
- Constitutional Foundation (Article 21):
- Mental Health as a Fundamental Right: The Court explicitly declared that mental health and psychological well-being are an integral component of the Right to Life and Dignity guaranteed under Article 21 of the Constitution.
- Structural Accountability: This ruling shifts mental health from a statutory right (under the Mental Healthcare Act, 2017) to a constitutional obligation, making the State and educational institutions accountable for systemic failures that lead to student distress.
- Key Binding Guidelines (Saha Guidelines): The Court issued binding directives for all educational institutions, hostels, and coaching centres, which hold the force of law under Article 141 until Parliament legislates.
| Directive Category |
Core Mandate |
|
|
- Institutions with 100+ students must appoint at least one qualified counsellor/psychologist. Smaller institutions must establish referral linkages.
|
|
|
- Banning public shaming, batch segregation based on performance, and assigning disproportionate academic targets.
|
|
|
- Mandatory bi-annual training for all staff in Psychological First Aid, identification of distress signs, and non-discriminatory support (especially for SC/ST, OBC, and LGBTQ+ students).
|
|
|
- Mandatory installation of tamper-proof ceiling fans in residential facilities and restriction of access to high-risk areas (rooftops).
|
|
|
- Mandated creation of confidential grievance redressal systems for discrimination and harassment, holding administrations liable for institutional culpability if neglect leads to self-harm.
|
|
Key Global Initiatives for Suicide Prevention
| Initiative |
Core Focus & Key Interventions |
India’s Relevance/Gap |
| WHO’s LIVE LIFE Package |
- The global, evidence-based roadmap for national strategies.
- Four Core Actions (L-I-F-E):
- Limit access to means (Tamper-proof fans, firearms, pesticides).
- Interact with media (Papageno Effect over Werther Effect).
- Foster life-skills (Social and Emotional Learning (SEL) in schools).
- Early identification (Gatekeeper training and follow-up).
- Six Foundational Pillars:
- Situation analysis (Data collection and surveillance).
- Multisectoral Collaboration (Involving health, education, labor, media, and justice sectors).
- Awareness raising and advocacy.
- Capacity building (Training staff and the community).
- Financing (Allocating adequate budget).
- Surveillance, monitoring, and evaluation.
|
- Blueprint for India’s National Suicide Prevention Strategy (NSPS).
- Directly influences National Suicide Prevention Strategy’s (NSPS) goals for curriculum, community training, and media guidelines.
- Highlights the critical need for inter-ministerial cooperation and increasing the 0.5% mental health budget.
|
| UN Sustainable Development Goals (SDG) |
- Target 3.4: Reduce premature mortality from Non-Communicable Diseases (NCDs) (including suicide) by one-third (33%) by 2030.
|
- India’s NSPS target (10% reduction by 2030) is significantly less ambitious than the global SDG target, demanding accelerated effort and investment.
|
| Academic & Institutional (WHO/WMH) |
- World Mental Health International College Student (WMH-ICS) Initiative: Global research on college students to develop cost-effective, web-based interventions.
- International Association for Suicide Prevention (IASP): Global Non-Governmental Organization (NGO) advocating for research, crisis systems, and decriminalization of suicide.
|
- Provides the scientific basis for digital and tele-counselling services (like Tele Mental Health Assistance and Networking Across States (Tele-MANAS)) and influenced the decriminalization of suicide in India (Mental Healthcare Act (MHCA) 2017).
|
| WHO-UNICEF Joint Program |
- Helping Adolescents Thrive: Focuses on strengthening the health and education system’s capacity to address adolescent (10-19 years) mental health needs and prevent self-harm.
|
- Reinforces the need to start prevention at the school level (9–17 age group), a key vulnerability area for India.
|
Systemic Barriers Undermining India’s Fight Against Student Suicides
- Policy Implementation & Governance Gaps: The biggest hurdle is the failure to translate judicial mandates and national strategies into effective action, primarily due to poor compliance and low funding.
- Critical Compliance Gaps: Only an estimated 40-50% of schools meet the Supreme Court’s order to appoint a qualified counselor.
- This non-compliance is particularly high in private coaching hubs, allowing harmful practices like public shaming and batch segregation to continue.
- Severe Underfunding: Mental health receives only a tiny 0.5% of India’s health budget.
- This gross underfunding makes it impossible to effectively carry out national plans, scale up infrastructure, or hire necessary professionals.
- Efficacy vs. Targets: The National Suicide Prevention Strategy (NSPS) target of a 10% reduction by 2030 is highly ambitious given the current rising trend and weak implementation.
- Furthermore, the low penetration of Tele-MANAS in rural areas undermines its efficacy despite handling millions of calls.
- Weak Inter-Ministerial Coordination: Effective prevention requires streamlined cooperation between Health, Education, and Social Justice ministries, which remains a consistent governance challenge.
- Challenges in Putting Plans into Action: Most schools lack safe spaces for confidential disclosure, dedicated mental-health budgets, and robust evidence-based emotional-literacy programmes.
- Institutional & Cultural Barriers: The prevailing academic culture actively contributes to the crisis by normalizing stress and lacking institutional ethics.
- Normalization of Toxicity: There is a deep-seated cultural acceptance of punitive discipline and extreme academic pressure, often mislabeled as “tough love.” This fosters self-stigma and prevents students from seeking help.
- Focus on Rote Learning: The hyper-competitive exam culture (NEET/JEE) prioritizes marks over holistic development, directly increasing student anxiety and the risk of suicide.
- Lack of Institutional Accountability: Before recent judicial mandates, there were few mechanisms to hold institutional administrations legally liable for negligence (e.g., failure to provide a mandated counselor).
- Data, Digital, & Contagion Risks: Modern threats—from poor surveillance to digital exposure—present new challenges to prevention efforts.
- Fragmented Data and Monitoring: Reliable data beyond the basic NCRB figures is fragmented, impeding targeted, evidence-based policy-making and accurate surveillance of high-risk clusters.
- Digital Overload & Contagion: Constant digital pressure, coupled with unregulated or sensationalized media coverage of student suicides, can lead to cluster suicides or imitation (Werther Effect), a risk that is difficult to monitor and contain.
- Intersectional Vulnerabilities: Systemic inequities ensure that marginalized groups bear a disproportionate burden of the crisis.
- Discrimination and Exclusion: Students from SC/ST/OBC backgrounds face significantly higher risks due to caste-based discrimination and economic precarity, which are often overlooked by general support programs.
- Gender and Identity Stigma: High patriarchal expectations on female students and extreme social stigma faced by LGBTQ+ youth create acute vulnerabilities that require specialized and sensitive interventions that are currently lacking.
Way Forward
Tackling the crisis requires a non-negotiable commitment to a holistic, structural reform, securing India’s future.
- Structural Reform: Addressing the student suicide crisis requires comprehensive structural changes across all levels, ensuring India’s future workforce and well-being are safeguarded.
- Accountability and School Reform: Judicial enforcement must be swift, with Institutional Culpability holding schools legally accountable for neglect, including failing to hire counsellors.
- Curriculums must focus on holistic assessment and mandatory Social and Emotional Learning to reduce exam-related stress.
- Programs like Tamil Nadu’s Happiness Curriculum and Kerala’s Student Police Cadet and Operation Sukoon show ten to fifteen percent lower distress, offering scalable models.
- State governments must rigorously enforce the Coaching Center Regulation Guidelines (2024), particularly banning practices like segregation, mandatory hostel stays, and admission below the age of 16 to reduce competitive pressure on younger students.
- Schools must mandatorily set up child protection committees under the Juvenile Justice (JJ) Act and Protection of Children from Sexual Offences (POCSO) norms to conduct periodic safety audits.
- Replace high-stakes exams with phased assessments and project-based learning, shifting the focus from rote memorization to holistic mastery… To mitigate acute pre-exam stress, schools must limit homework, regulate coaching pressure, and create mandatory buffer days around exam schedules.
- Teacher and Community Empowerment: Psychological First Aid training should be mandatory for all teachers.
- Parents, Accredited Social Health Activist workers, and Anganwadi workers must be trained as community gatekeepers, reducing risk and providing early support.
- International models, such as Finland, demonstrate twenty-five percent reductions in youth suicides through community engagement.
- Innovation and Multi-Sectoral Governance: Cooperation between the Ministry of Education and Ministry of Health and Family Welfare is critical.
- Corporate Social Responsibility funds can support infrastructure safety, while Artificial Intelligence chatbots and predictive analytics can detect early warning signs.
- Responsible media reporting can prevent imitative suicides, replicating the Papageno effect, with ten to thirteen percent reductions observed internationally.
- The Ministry of Education, in collaboration with the Ministry of Electronics and Information Technology (MeitY), must finalize Digital Safety Guidelines and promote digital detox programs to regulate screen time and manage online academic anxiety.
Conclusion
As Mahatma Gandhi said, “there is no school equal to a decent home and no teacher equal to a virtuous parent.” The State must act as the virtuous parent, protecting children from preventable despair. Every day, India loses thirty-eight bright young lives.
- If unaddressed, this silent epidemic will erode 8–10 years of India’s demographic dividend window, making Viksit Bharat @2047 impossible without urgent, mission-mode reform. Only when education truly liberates rather than suffocates will Tagore’s heaven of freedom truly dawn.


 9 Dec 2025
9 Dec 2025



.png)



 Current Affairs
Current Affairs


 GS Foundation
GS Foundation Optional Course
Optional Course Combo Courses
Combo Courses Degree Program
Degree Program